The main pathophysiologic characteristic in individuals with progressive familial intrahepatic cholestasis (PFIC) is a defect in bile secretion. These patients typically present with cholestasis, usually in infancy and childhood.1
It is important to note that while PFIC is generally caused by a defect in bile secretion, the mechanism behind each subtype differs slightly.
The exact mechanism of cholestasis and other symptoms in PFIC1 is unknown. The proposed mechanism, however, includes an overload of bile acid in hepatocytes due to reduced bile salt secretion and increased ileal bile salt reabsorption.
This overload occurs due to downregulation of farnesoid X receptor (FXR), which is a receptor that regulates bile acid homeostasis.
This, in turn, results in:
Downregulation of bile salt export pump (BSEP) proteinUpregulation of synthesis of bile acids in the hepatocytesUpregulation of ileal bile acid transporter (IBAT) in the small intestine
BSEP is a transporter protein, expressed at the canalicular membrane of hepatocytes. It is the main exporter of bile acids from hepatocyte to canaliculi against a concentration gradient. As a result of genetic mutations, there can be defective processing or trafficking of BSEP transporter proteins, or a disruption of the structure or functional domain of BSEP transporter proteins.
These defects in BSEP synthesis and/or function lead to bile secretion, followed by:
Decreased bile flowAccumulation of bile acids in hepatocytesHepatocellular damage
In PFIC3, a defect in the ABCB4 gene encoding leads to defects in the multidrug resistance class III (MDR3) protein, which is responsible for the biliary secretion of phospholipids. Phospholipids are responsible for neutralizing the detergent effects of bile acids, so the defects in MDR3 result in injury of biliary epithelium and bile canaliculi—ultimately, leading to cholestasis.
Serum Bile Acids
An important component of bile are bile acids, which help facilitate digestion and absorption of dietary cholesterol, triglycerides, and fat-soluble vitamins.3
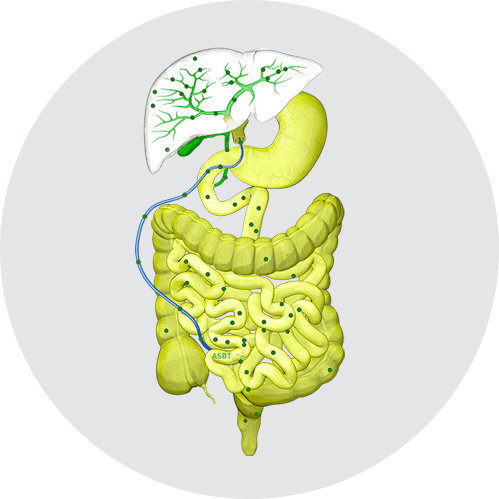
NORMAL ENTEROHEPATIC CIRCULATION
Normally, bile acids are synthesized in hepatocytes and secreted in the bile via bile salt export pumps (BSEP) at the apical (canalicular) membrane. Bile acids then move through bile ducts to the gallbladder for storage and, later, for release into the small intestine to aid in digestion and absorption. Per cycle, up to 95% of bile acids are reabsorbed from the ileum via the apical sodium-dependent bile acid transporter (ASBT), also known as the ileal bile acid transporter (IBAT), for return to the liver through the hepatic portal vein.4
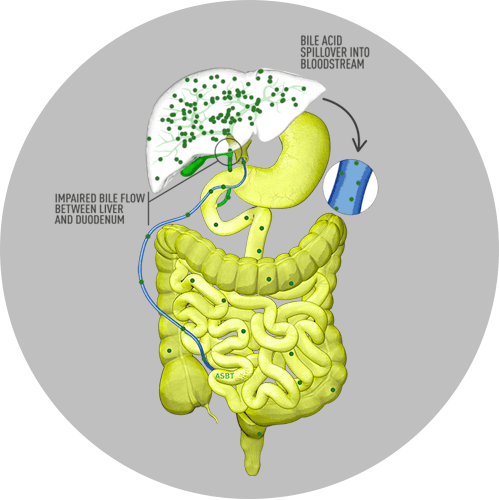
CHOLESTATIC LIVER DISEASE MECHANISM OF DISEASE
In cholestatic liver disease, the flow of bile is impaired at some point between the liver cells, which produce bile, and the duodenum. Bile acids, therefore, build up in the liver. This leads to liver injury and/or progressive liver disease, and, if left untreated, can result in fibrosis, cirrhosis, liver failure, and death. In addition, there is spillover of bile into the bloodstream, resulting in increased serum bile acids (sBA).5,6
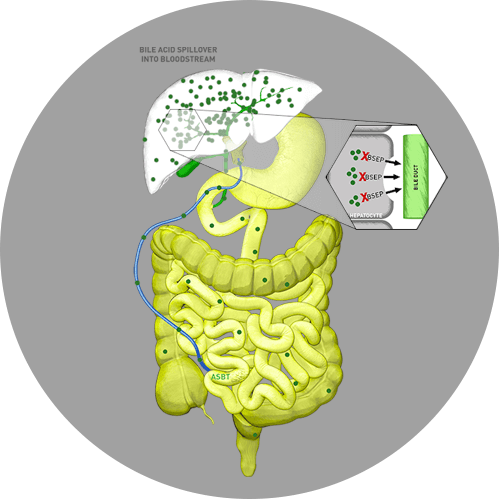
PFIC MECHANISM OF DISEASE
In progressive familial intrahepatic cholestasis (PFIC), specifically, the liver is unable to secrete bile acids as the result of a genetic defect. With fewer functional BSEP transporters, hepatocytes are unable to push out bile into the bile ducts. As a result, bile accumulates to high levels in the liver and in the bloodstream.1,7 All 3 subtypes of PFIC present with elevated sBA—nearly 10- to 20-fold elevations—with extremely elevated levels in PFIC2.7-9
Treatment interventions, such as partial external biliary diversion (PEBD) surgery in patients with PFIC, aim to reduce levels of circulating bile acids and, therefore, improve pruritus.10
Pruritus
Cholestatic pruritus is a debilitating symptom, often resulting in a significant reduction in quality of life.1 For children and their parents, cholestatic pruritus is an extremely distressing manifestation of progressive familial intrahepatic cholestasis (PFIC)—and its relief is often the goal of early therapy.7
Pruritus is reported as a primary symptom in
11% to 100%
of patients at presentation10
76% to 100%
of patients at follow-up10
Based on the Whitington scale (0, none; 1+, rubbing or mild scratching when not distracted; 2+, active scratching without evident skin abrasions; 3+, abrasions evident; 4+, cutaneous mutilation, hemorrhage, and scarring evident)10:
Pruritus is reported to be often severe (grade 3+ or 4+) in
76% to 80%
of patients10
Pruritus is associated with abrasions, cutaneous mutilation, hemorrhage, and scarring, and leads to significantly diminished quality of life—assessed using the Pediatric Quality of Life Inventory (PedsQL)—in patients with PFIC compared with healthy peers.10
In a group of children with chronic intrahepatic cholestasis, including those with PFIC, PedsQL self-reported scores were lower than in those of healthy controls (73 vs 84; effect size, 0.87).10 The degree of cholestasis, as measured by elevated total bilirubin, was associated with lower summary scores of health-related quality of life (HRQoL) by child self-report.11
Intractable pruritus can cause severe sleep deprivation and exhaustion, resulting in fatigue, depression, and impaired school performance.1,12
In PFIC, cholestasis can present with pruritus as a result of the accumulation of sBA.4
The goal of medical management is to provide relief from pruritus, improve the nutritional status, correct vitamin deficiencies, and treat complications of advanced liver disease. Due to disease management shortcomings, PEBD aims to reduce levels of circulating bile acids and improve pruritus.1
For patients with PFIC, PEBD relieved pruritus in only 54%.13
More specifically, in a retrospective analysis of 24 patients with PFIC undergoing PEBD, 54% improved significantly, with a normalization of sBA (P<.001 vs preoperatively) and lessened pruritus (P<.05 vs preoperatively) at 12 months after PEBD.14
In a study of 24 patients with PFIC who underwent PEBD, bile acid levels decreased in 10 patients with PFIC1 (1724 ± 3215 μmol/L to 11 ± 6 μmol/L, P=0.03) and in a single patient with PFIC3 (821 μmol/L to 11 μmol/L), but not significantly in 13 patients with PFIC2 (193 ± 99 μmol/L to 141 ± 118 μmol/L, P=0.15).15
NAPPED (NAtural course and Prognosis of PFIC and Effect of biliary Diversion) is the largest global database of genotyped patients with BSEP deficiency. NAPPED aims to characterize the natural history of severe BSEP deficiency and to assess the effect of genetic, clinical, and therapeutic parameters on major surgical and clinical events, such as native liver survival (NLS), liver transplant, and mortality.13
From a recent retrospective cohort of patients with PFIC2 from the NAPPED database13:
of patients presented with pruritus
After surgical biliary diversion (SBD):
had no improvement of pruritushad transient partial or complete relief of pruritushad sustained partial or complete relief of pruritus
SBD was associated with significantly increased NLS (hazard ratio 0.50; 95% CI: 0.27–0.94; P=0.03) in BSEP1 and BSEP2. An sBA concentration below 102/mol/L or a decrease of at least 75%, each shortly after SBD, reliably predicted NLS of ≥15 years following SBD (each P<0.001).
The most debilitating symptom of cholestasis in PFIC is intense pruritus, which is among the worst in any cholestatic liver disease.16
Due to a lack of pediatric itch assessments that meet current FDA patient-reported outcome (PRO) guidelines, the Itch Reported Outcome (ItchRO) tool—available as both a patient- and caregiver-reported outcome tool—was developed specifically for, and fully validated in, patients with cholestatic liver disease.17
ItchRO Tool
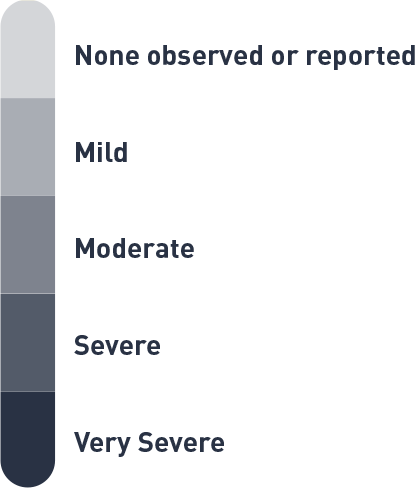
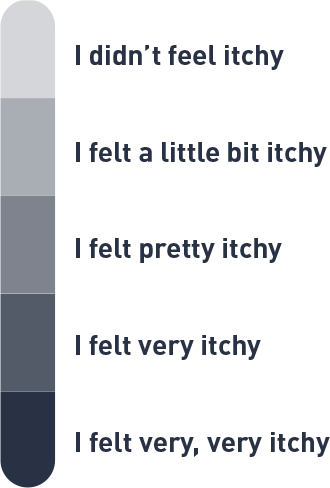
The ItchRO tool features a 5-point scoring system to assess the intensity of the itching18:
Move the slider to view the itch scale.
0=None
1=Mild Itch
2=Moderate Itch
3=Severe Itch
4=Very Severe Itch
Move the slider to view the itch scale.
0=None
1=Mild Itch
2=Moderate Itch
3=Severe Itch
4=Very Severe Itch
In practice, a caregiver is provided with a morning and evening ItchRO electronic diary18:
Morning Diary Example
Based on observations or what your child told you about his/her itching, how severe were your child's itch-related symptoms (rubbing, scratching, skin damage, sleep disturbances, or irritability) from when he/she went to bed last night until he/she woke up this morning?
Evening Diary Example
Based on observations or what your child told you about his/her itching, how severe were your child's itch-related symptoms (rubbing, scratching, skin damage, sleep disturbances, or irritability) from the time he/she woke up this morning until he/she went to bed?
A patient who is ≥9 years of age, on the other hand, is provided with morning and evening diaries that differ slightly17:
ItchRO: Morning Diary Example
Think about whether itching kept you awake or woke you up last night. Think about whether you felt like rubbing or scratching.
How itchy did you feel last night after you went to bed until you woke up this morning?
(Note: The following two items are exploratory and will not contribute to the ItchRO score. If the subject answered “I didn’t feel itchy”, the following will not be presented on the eDiary)
Did feeling itchy make it hard to fall asleep last night?
Yes
No
Did feeling itchy wake you up last night?
Yes
No
ItchRO: Evening Diary Example
Think about how itchy you were all day. Think about whether you felt like rubbing or scratching.
How itchy were you all day today from the time when you woke up until now?
(Note: The following item is exploratory and will not contribute to the ItchRO score. If the subject answered “I didn’t feel itchy”, the following will not be presented on the eDiary)
Did feeling itchy make you rub or scratch today?
No
Yes, but it left no marks
Yes, and it left marks but my skin wasn’t red
Yes, and it left red marks
Yes, and my skin bled
Clinician Scratch Scale (CSS)
In addition to the caregiver- and patient-rated ItchRO, pruritus can also be assessed using the physician-rated CSS score.19
The CSS is based on a 5-point scale, where19,20:
none
rubbing or mild scratching when undistracted
active scratching without evident skin abrasions
abrasions evident
cutaneous mutilation, hemorrhage, and scarring evident
These novel tools allow physicians to better assess the severity of itching in children with PFIC and other cholestatic liver diseases.
ASBT=apical sodium-dependent bile acid transporter; BSEP=bile salt export pump; CSS=Clinician Scratch Scale; FXR=farnesoid X receptor; HRQoL=health-related quality of life; IBAT=ileal bile acid transporter; ItchRO=Itch Reported Outcome; MDR3=multidrug resistance class III; NLS=native liver survival; PEBD=partial external biliary diversion; PedsQL=Pediatric Quality of Life Inventory; PFIC=progressive familial intrahepatic cholestasis; PRO=patient-reported outcome; sBA=serum bile acid; SBD=surgical biliary diversion.
References:1. Srivastava A. Progressive familial intrahepatic cholestasis. J Clin Exp Hepatol. 2014;4(1):25-36. doi:10.1016/j.jceh.2013.10.005 2. Stofan M, Guo GL. Bile Acids and FXR: Novel Targets for Liver Diseases. Front Med (Lausanne). 2020;7:544. doi:10.3389/fmed.2020.00544 3. Di Ciaula A, Garruti G, Lunardi Baccetto RL, et al. Bile acid physiology. Ann Hepatol. 2017;16(suppl 1):s4-s14. doi:10.5604/01.3001.0010.5493 4. Kamath BM, Stein P, Houwen RHJ, Verkade HJ. Potential of ileal bile acid transporter inhibition as a therapeutic target in Alagille syndrome and progressive familial intrahepatic cholestasis. Liver Int. 2020;40(8):1812-1822. doi:10.1111/liv.14553 5. Chiang JYL, Ferrell JM. Bile acid metabolism in liver pathobiology. Gene Expr. 2018;18(2):71-87. doi:10.3727/105221618X15156018385515 6. Jones EA, Bergasa NV. The pruritus of cholestasis: from bile acids to opiate agonists. Hepatology. 1990;11(5):884-887. doi:10.1002/hep.1840110526 7. Gunaydin M, Bozkurter Cil AT. Progressive familial intrahepatic cholestasis: diagnosis, management, and treatment. Hepat Med. 2018;10:95-104. doi:10.2147/HMER.S137209 8. Jericho HS, Kaurs E, Boverhof R, et al. Bile acid pool dynamics in progressive familial intrahepatic cholestasis with partial external bile diversion. J Pediatr Gastroenterol Nutr. 2015;60(3):368-374. doi:10.1097/MPG.0000000000000630 9. Medscape. Progressive familial intrahepatic cholestasis. Updated April 26, 2017. Accessed March 9, 2021. https://emedicine.medscape.com/article/932794-overview 10. Baker A, Kerkar N, Todorova L, Kamath BM, Houwen RHJ. Systematic review of progressive familial intrahepatic cholestasis. Clin Res Hepatol Gastroenterol. 2019;43(1):20-36. doi:10.1016/j.clinre.2018.07.010 11. Kamath BM, Chen Z, Romero R, et al. Quality of life and its determinants in a multicenter cohort of children with Alagille syndrome. J Pediatr. 2015;167(2):390-396.e3. doi:10.1016/j.jpeds.2015.04.077 12. Düll MM, Kremer AE. Newer approaches to the management of pruritus in cholestatic liver disease. Curr Hepatol Rep. 2020;19:86-95. doi:10.1007/s11901-020-00517-x 13. van Wessel DBE, Thompson RJ, Gonzales E, et al. Genotype correlates with the natural history of severe bile salt export pump deficiency. J Hepatol. 2020;73(1):84-93. doi:10.1016/j.jhep.2020.02.007 14. Schukfeh N, Metzelder ML, Petersen C, et al. Normalization of serum bile acids after partial external biliary diversion indicates an excellent long-term outcome in children with progressive familial intrahepatic cholestasis. J Pediatr Surg. 2012;47(3):501-505. doi:10.1016/j.jpedsurg.2011.08.010 15. Lemoine C, Bhardwaj T, Bass LM, Superina RA. Outcomes following partial external biliary diversion in patients with progressive familial intrahepatic cholestasis. J Pediatr Surg. 2017;52(2):268-272. doi:10.1016/j.jpedsurg.2016.11.021 16. Ayoub MD, Kamath BM. Alagille syndrome: diagnostic challenges and advances in management. Diagnostics (Basel). 2020;10(11):907. doi:10.3390/diagnostics10110907 17. Kamath BM, Abetz-Webb L, Kennedy C, et al. Development of a novel tool to assess the impact of itching in pediatric cholestasis. Patient. 2018;11(1):69-82. doi:10.1007/s40271-017-0266-4 18. Kamath BM, Spino C, McLain R, et al. Unraveling the relationship between itching, scratch scales, and biomarkers in children with Alagille syndrome. Hepatol Commun. 2020;4(7):1012-1018. doi:10.1002/hep4.1522 19. Kamath BM, Ye W, Goodrich NP, et al. Outcomes of childhood cholestasis in Alagille syndrome: results of a multicenter observational study. Hepatol Commun. 2020;4(3):387-398. doi:10.1002/hep4.1468 20. Whitington PF, Whitington GL. Partial external diversion of bile for the treatment of intractable pruritus associated with intrahepatic cholestasis. Gastroenterology. 1988;95(1):130-136. doi:10.1016/0016-5085(88)90301-0